If you have allergic asthma, you know the drill. You take your inhaler when things get tight, maybe bump up your daily medication during pollen season, and hope for the best. But what if there was a way to actually change how your immune system reacts to allergens, rather than just masking the symptoms? That is exactly what allergen immunotherapy is a disease-modifying treatment that gradually desensitizes the immune system through controlled exposure to specific allergens. It is currently the only medical approach that targets the root cause of IgE-mediated allergic conditions like asthma, rather than just suppressing inflammation temporarily.
The big question most patients face is not whether it works-evidence shows it does-but which method is right for them. Do you go with the traditional route of subcutaneous immunotherapy (SCIT), commonly known as allergy shots? Or do you try the newer, home-based option of sublingual immunotherapy (SLIT) using tablets or drops? The choice isn't just about preference; it involves weighing efficacy, safety, convenience, and long-term commitment. Let's break down what the latest clinical data tells us about these two approaches so you can make an informed decision with your doctor.
How Allergen Immunotherapy Actually Works
To understand why either shots or tablets might help your asthma, you first need to grasp the mechanism behind immunotherapy. Unlike antihistamines or inhaled corticosteroids, which treat the aftermath of an allergic reaction, immunotherapy retrains your immune system. Think of it like teaching your body to ignore a false alarm.
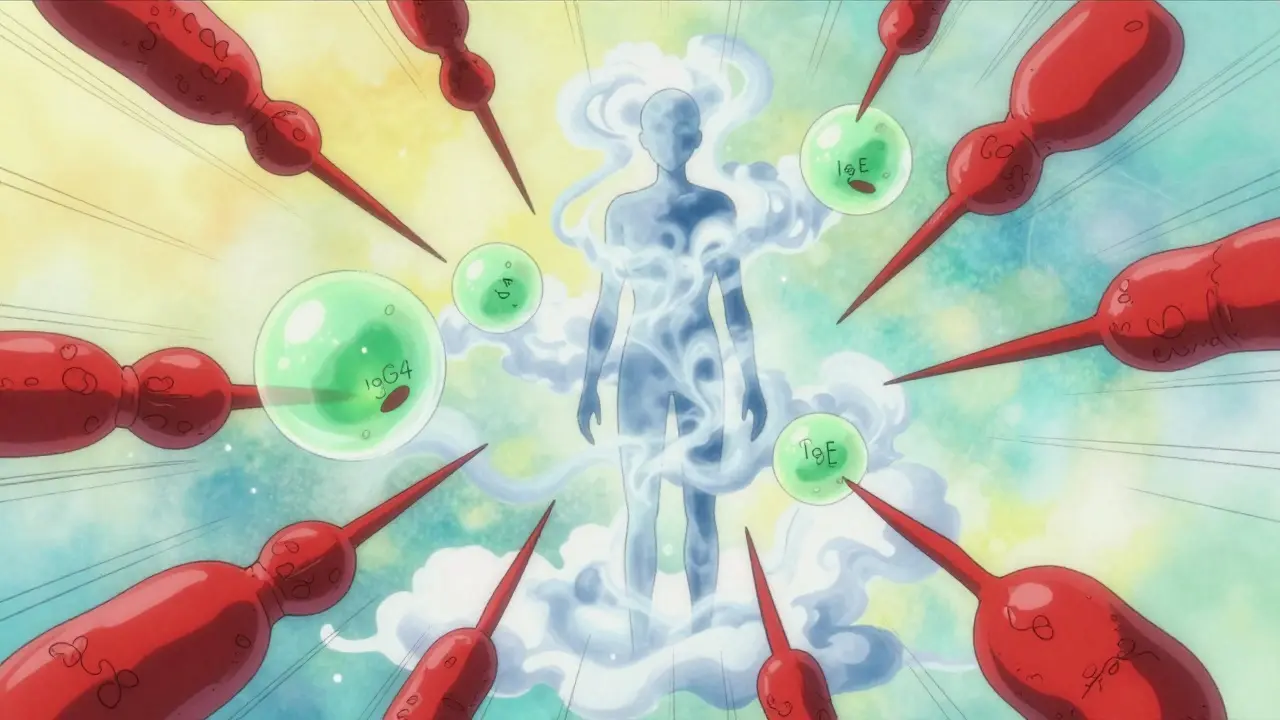
Immunotherapy works by administering gradually increasing doses of a specific allergen over time to build tolerance. When you are allergic to house dust mites or grass pollen, your immune system overreacts, releasing histamine and other chemicals that cause swelling, mucus, and bronchoconstriction. By exposing you to tiny, controlled amounts of that allergen regularly, the therapy shifts your immune response. It encourages the production of blocking antibodies (IgG4) while reducing the activity of the IgE antibodies that trigger symptoms. This process takes time-typically three to five years-but the goal is lasting relief even after you stop treatment.
The concept dates back to 1911, when doctors Leonard Noon and John Freeman first introduced subcutaneous injections of pollen extracts. Since then, the science has evolved significantly. Today, guidelines from the European Academy of Allergy and Clinical Immunology (EAACI) confirm that this approach modifies the underlying pathophysiology of allergic diseases. For asthma specifically, this means fewer exacerbations, less reliance on rescue medications, and potentially preventing the progression from allergic rhinitis (hay fever) to full-blown asthma.
Subcutaneous Immunotherapy (SCIT): The Traditional Shot
When people think of "allergy shots," they are thinking of SCIT. This is the gold standard against which newer methods are often measured. Here is how it works in practice.
Subcutaneous Immunotherapy (SCIT) involves regular injections administered under the skin in a clinical setting, following a strict build-up and maintenance schedule. The process is divided into two phases. First, there is the build-up phase, where you receive weekly injections for three to six months. During this time, the dose increases incrementally until you reach a target level. Then comes the maintenance phase, where you switch to monthly injections for the remaining two to four years of treatment.
The biggest advantage of SCIT is its track record. A landmark study by Dr. D. Mungan in 1999 involving mite-sensitive patients showed that SCIT effectively reduced both rhinitis and asthma symptoms. Because the injections are given in a clinic, medical professionals can monitor you for immediate reactions, providing a high level of safety control. Additionally, because you don't have to remember to take a pill every day, adherence issues related to forgetfulness are eliminated-you show up, you get the shot, you leave.
However, the downside is obvious: inconvenience. Over a three-year course, you will likely visit the clinic around 50 times. Each visit requires waiting periods (usually 30 minutes) to ensure no severe systemic reaction occurs. For busy professionals or parents with young children, finding time for bi-monthly appointments can be a significant hurdle. Furthermore, injection site reactions-redness, swelling, and itching-are common, though usually mild.
Sublingual Immunotherapy (SLIT): The Tablet Option
SLIT offers a different pathway to desensitization. Instead of needles, you place a tablet or drop under your tongue. After holding it there for about two minutes, you swallow it. The mucous membranes under the tongue absorb the allergen, triggering the same immune-modulating effects as injections but through a different route.
Sublingual Immunotherapy (SLIT) utilizes standardized allergen tablets or drops taken daily at home after initial medical supervision. Common approved products include GRAZAX for grass pollen and ACARIZAX for house dust mites. These are standardized to specific units (like 6 SQ-HDM for house dust mite) to ensure consistent dosing.
The primary benefit here is convenience and safety. You take the first dose in the doctor's office to rule out severe reactions, but after that, you administer the rest at home. No more driving to the clinic every month. Recent real-world evidence strongly supports this method. A 2024 analysis by Dr. C. Asperti highlighted that patients receiving the highest dose of house dust mite SLIT achieved an 81 μg reduction in their daily inhaled corticosteroid (ICS) dose compared to placebo. That translates to a relative mean ICS reduction of 42%, compared to just 15% for those on placebo. In simpler terms, patients needed significantly less steroid medication to keep their asthma under control.
Adherence rates for SLIT are generally higher (around 75-80%) compared to SCIT (60-65%) simply because it fits into daily life more easily. However, local side effects like oral itching or throat tickling are common in the first few weeks, though they typically resolve as your body adjusts.
Head-to-Head Comparison: Efficacy and Safety
So, which one is better? The answer depends on what you value more: maximum proven efficacy for severe cases or convenience and lifestyle integration. Let's look at the data side-by-side.
| Feature | SCIT (Shots) | SLIT (Tablets) |
|---|---|---|
| Administration | Subcutaneous injection in clinic | Tablet under tongue at home |
| Frequency | Weekly (build-up), then Monthly | Daily |
| Duration | 3-5 years | 3-5 years |
| Clinic Visits | ~50 visits over 3 years | Initial dose + periodic check-ups |
| Efficacy (Asthma) | High, established long-term data | Comparable, strong recent RCT support |
| Safety Profile | Higher risk of systemic reactions | Very low risk of systemic reactions |
| Medication Reduction | Significant reduction in controllers/relievers | Up to 42% reduction in ICS dose (HDM SLIT) |
| Best For | Multiple allergens, needle-tolerant patients | Single allergen (e.g., HDM, Grass), busy schedules |
Historically, some older studies suggested SCIT was slightly more effective for asthma symptom control. However, modern randomized controlled trials (RCTs) and large-scale register studies have narrowed that gap considerably. A propensity-matched study of over 14,000 patients found that AIT-treated individuals had significantly greater reductions in prescriptions for both rhinitis and asthma medications compared to controls, with benefits sustained over nine years. Specifically for SLIT, a nationwide study of 2,688 patients showed a 20% decrease in lower respiratory tract infections requiring antibiotics among perennial allergic asthmatics after treatment discontinuation.
Safety is where SLIT shines brightest. Systemic reactions (whole-body allergic responses) are rare with SLIT and almost always mild. With SCIT, while still rare, the risk is higher, which is why the 30-minute wait in the clinic is mandatory. If you have a fear of needles or live far from an allergy specialist, SLIT removes those barriers entirely.
Who Is a Candidate for Immunotherapy?
Not everyone with asthma qualifies for allergen immunotherapy. It is crucial to manage expectations here. This treatment is designed for specific profiles:
- Allergen-Specific Triggers: Your asthma must be triggered by identifiable allergens such as house dust mites, grass pollen, tree pollen, or cat dander. If your asthma is triggered by exercise, cold air, or viruses, immunotherapy will not help.
- Mild to Moderate Asthma: Candidates typically fall into GINA steps 1-3. If you have severe, uncontrolled asthma (GINA steps 4-5), immunotherapy is generally contraindicated until your condition is stabilized with medication.
- Confirmed Sensitivity: You must have positive results from skin prick tests or specific IgE blood tests confirming sensitivity to the allergen you plan to treat.
- Inadequate Control with Medication Alone: If you are already well-controlled on low-dose inhalers and have minimal symptoms, the hassle of immunotherapy might not be worth it. It is most valuable for those who struggle with current treatments or want to reduce their medication burden long-term.
Conversely, if you have non-allergic asthma, severe cardiovascular disease, or are taking beta-blockers (which can complicate the treatment of allergic reactions), you may not be a suitable candidate. Always discuss your full medical history with an allergist.

Practical Considerations: Cost, Access, and Adherence
Beyond the biology, practical realities play a huge role in success. Let's talk about the logistics.
Adherence is Key. Immunotherapy is a marathon, not a sprint. Missing doses reduces efficacy. With SCIT, missing a monthly appointment happens, but the structure is rigid. With SLIT, the responsibility falls entirely on you. Can you commit to taking a pill every single morning for three years? Studies show SLIT adherence is good (75-80%), but it requires discipline. Setting phone alarms or linking it to another daily habit (like brushing teeth) helps.
Geographic Availability. There is a significant transatlantic divide in access. In Europe, SLIT products like ACARIZAX and GRAZAX are widely approved and reimbursed. In the United States, FDA-approved options are more limited, and insurance coverage can be spotty. According to industry analysis, approximately 60-70% of European allergists offer SLIT, compared to only 10-15% in the US. If you are in the US, check with your insurance provider early to see if they cover off-label use of certain tablets or if they prefer SCIT.
Cost Savings. While immunotherapy has upfront costs, it can save money over time. The 2024 study noting a 42% reduction in inhaled corticosteroids suggests substantial savings on prescription drugs. Fewer exacerbations also mean fewer emergency room visits and lost work days. Over a decade, the investment often pays for itself.
Next Steps: How to Start
If you think immunotherapy might be right for you, here is your action plan:
- Get Tested: Schedule an appointment with a board-certified allergist. Request comprehensive skin prick testing or specific IgE blood tests to identify your exact triggers.
- Review Your Asthma Control: Ensure your asthma is stable. If you are having frequent attacks, work with your doctor to optimize your controller medications first.
- Discuss Options: Ask your doctor specifically about both SCIT and SLIT. Mention your lifestyle constraints. Do you travel frequently? Are you needle-phobic? Do you have trouble remembering daily tasks?
- Check Insurance: Call your insurer to ask about coverage for "allergen immunotherapy" and specify whether they cover sublingual tablets or only injections.
- Commit to the Timeline: Understand that you won't feel immediate relief. Benefits usually start appearing after 3-6 months, with optimal results after 1-2 years. Plan for a 3-5 year commitment.
How long does it take for allergen immunotherapy to work for asthma?
Most patients begin to notice improvements in symptoms and reduced medication needs within 3 to 6 months of starting treatment. However, the full therapeutic benefit, including long-term desensitization, typically requires completing the entire 3 to 5-year course. Stopping early may result in temporary relief that fades once treatment ceases.
Can SLIT tablets cure asthma permanently?
Immunotherapy is considered "disease-modifying" rather than curative. While it cannot guarantee a permanent cure, many patients experience long-term remission of symptoms even after stopping treatment. Studies show that benefits can last for several years post-treatment, and some patients never require further allergy medication.
Is it safe to use SLIT if I have severe asthma?
Generally, no. Patients with severe, uncontrolled asthma (GINA steps 4-5) are not candidates for immunotherapy until their condition is stabilized with appropriate medication. Starting immunotherapy during a period of poor control increases the risk of serious adverse reactions. Always consult your allergist for a personalized risk assessment.
What are the common side effects of allergy shots vs. tablets?
SCIT (shots) commonly causes local reactions like redness, swelling, and itching at the injection site. Rarely, systemic reactions like hives or breathing difficulties can occur, which is why observation in a clinic is required. SLIT (tablets) typically causes mild local irritation under the tongue, such as itching or tingling, which usually subsides within the first few weeks of treatment. Systemic reactions with SLIT are very rare.
Does insurance cover allergen immunotherapy?
Coverage varies significantly by region and provider. In many countries, especially in Europe, standardized SLIT products are widely reimbursed. In the US, coverage for SCIT is more common, while SLIT coverage depends on the specific product and insurance plan. It is essential to verify benefits and prior authorization requirements with your insurance company before starting treatment.





